Developing Guidelines for Admission, Triage, and Discharge Criteria for Cancer Patients in the Intensive Care Unit
An initiative of the Onco Critical Care Society (OCCS)
THE CHALLENGE
Admitting a critically ill cancer patient to the ICU is a complex decision at the intersection of oncology, critical care, and ethics. While historical pessimism persists, modern data show improved survival – yet significant variability in practice remains. No standardized, evidence‑based framework exists for this vulnerable population. OCCS is filling this gap.
STEERING COMMITTEE
Intensivists: Saurabh Kumar Das (India), Raymond Savio (India), Marlies Osterman (UK), Jose Garnacho (Spain), Ravi Jain (Methodologist, India), Ranvir Singh Tyagi (India), Bram Rochwerg (Canada), Pradip Tiwari, Amit Kansal (Singapore), Bruno L Ferreyro (Canada), Parveen Kaur (India)
Oncologists: Deepak George (India), Bhawana Sirohi (India)
Palliative Care: Veereswara Raju SK (India)
KEY OBJECTIVES
1. Develop explicit criteria and a procedural framework for admission, triage, and discharge of adult critically ill cancer patients.
2. Establish oncology‑specific triage principles for periods of system strain.
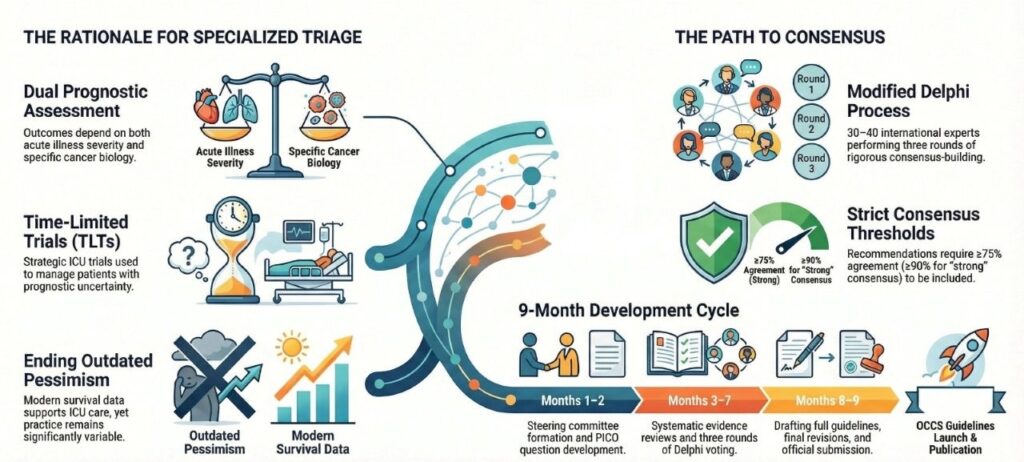
3. Define the use of “Time‑Limited Trials” (TLTs) for patients with prognostic uncertainty.
4. Provide clear criteria for safe ICU discharge – to ward, palliative care, or hospice.
WHY CANCER PATIENTS ARE DIFFERENT
• Dual prognostic assessment: acute illness severity + cancer biology (histology, stage, molecular markers, performance status)
• Reversibility depends on both organ recovery and response to cancer‑directed therapy
• Time‑limited trials are often appropriate for intermediate‑prognosis patients
• Unique oncologic emergencies: tumor lysis syndrome, SVC syndrome with airway compromise, hyperleukocytosis, spinal cord compression
• Discharge to palliative care is a distinct and important outcome
METHODOLOGY
Modified Delphi process: 3 rounds, ≥75% consensus (≥80% for MCQs). Steering committee + independent Delphi expert. 30–40 international experts (intensivists, oncologists, emergency physicians). Strong consensus (≥90% agreement or median 6‑7) vs. weak consensus (≥75% but not strong). Stability testing (χ²), ACCORD reporting.
TIMELINE – 9 MONTHS
Months 1‑2: Steering committee, scope, PICO questions
Months 3‑5: Systematic reviews and evidence synthesis
Months 5‑6: Delphi round 1
Month 6: Analysis, revision, Delphi round 2
Month 7: Delphi round 3 (if needed)
Month 8: Draft full guideline
Month 9: Final revisions, submission
DISSEMINATION
Peer‑reviewed publication, OCCS website, one‑page infographic and algorithm, OCCS Annual Congress launch, webinars and newsletters.
OUTCOME
First‑ever evidence‑based, consensus‑driven recommendations for admission, triage, and discharge of cancer patients in the ICU – moving beyond the outdated “cancer vs. no cancer” dichotomy.